Latissimus dorsi flap reconstruction uses skin, fat and muscle from the back to recreate the breast mound. This tissue is tunneled to the breast region while remaining attached, or pedicled, to its donor site, so the blood supply remains intact. In some cases, the latissimus flap can reconstruct a complete breast mound, but often it provides the muscle and tissue necessary to cover and support an implant. The addition of the flap to the expander/implant gives Dr. Kim more control over the aesthetic appearance of the reconstructed breast. As with abdominally-based flaps, the latissimus flap helps create a more natural breast shape, projection and feel as opposed to an expander/implant alone. The latissimus flap is taken from the area below the shoulder and behind the armpit. Because this is a region with less fatty tissue than the abdomen, this reconstructive modality does often necessitate the placement of an expander or implant in conjunction with the flap to achieve the desired breast size. Whether or not a prosthesis is required is based on individual patients’ anatomies, which Dr. Kim assesses upon initial consultation visit to his Chicago office. Latissimus reconstruction is particularly useful as a salvage reconstruction technique after radiation and as an alternative in patients for whom abdominal flaps are not advised.
If an expander is placed along with the flap, the patient will come into Dr. Kim’s office in the Galter Pavilion of the Northwestern campus in downtown Chicago for expander fills approximately every week or every other week. Typically, because both a latissimus flap and an expander are in place to recreate the breast mound, fewer expansion will be necessary to achieve the desired size than if a patient has an expander alone. Then, in a second surgery, the expander is removed and a permanent implant is placed, as with tissue expander/implant reconstruction.
Check out Dr. Kim’s original article entitled “The utility of the tabbed expander in latissimus dorsi reconstruction” here.
The latissimus flap procedure adds approximately two to three hours onto the mastectomy surgery, and Dr. Kim usually has his patients remain in the hospital for 23 hours total, meaning the procedure is outpatient. During surgery, he will place one or more drains to release any fluid that collects in the newly reconstructed breast in the days or weeks following surgery. Normal recovery time is about three to four weeks. During office visits both before and after this surgery, Dr. Kim communicates with his patients about his expectations for decreased lifting and other activity after surgery, as well as any other restrictions he may want to impose to facilitate smooth recovery.
Secondary procedures are typically done about three months after the latissimus dorsi flap reconstruction. This includes exchange of the expander for a permanent implant, nipple reconstruction and other revision procedures to improve breast symmetry. Ideal candidates for the latissimus flap reconstruction process are thin, have a small breast volume and have excess tissue in their lateral breast area and in their mid-back region.
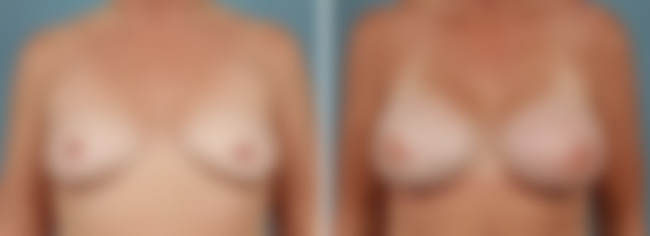
As Dr. Kim will discuss during your personalized breast reconstruction consultation visit to his Chicago office, the latissimus flap modality is a good option for women with a paucity of abdominal tissue but who desire autologous reconstruction (use of their own tissue to rebuild a breast mound after mastectomy). A major upside to latissimus reconstruction is that the flap remains attached to its native blood supply on the back, so the flap failure rate is quite low (flap failures result from interrupted blood supply). This procedure is also ideal for women with prior radiation to the chest, as radiation thins the skin among other issues, so flap coverage supports and strengthens the compromised area. If a woman has undergone radiation prior to her mastectomy surgery, the latissimus flap can be performed immediately at the time of the mastectomy. Similarly, if a patient has undergone prior breast surgery and has scarring, Dr. Kim will often opt for the latissimus reconstruction. Here is an example of one of Dr. John Kim’s patients who had radiation treatment prior to her mastectomies, so he performed the latissimus reconstruction at the time of the breast removal:
For women experiencing wound healing issues (i.e., a tissue expander was placed at the time of the mastectomy and is poking through the skin, or the incision is not healing) a latissimus flap is a good option for providing enough supportive tissue to prevent loss of the expander and a reconstructive failure. Additionally, if a patient experienced a complication from a first attempt at reconstruction (i.e., infection or mastectomy flap necrosis, meaning tissue death), the latissimus flap is an ideal form of secondary, or salvage, reconstruction.
Dr. Kim also utilizes something called a minimally invasive latissimus flap after a patient has had a lumpectomy. He creates a small incision under the armpit, one that is normally quite small and unnoticeable. The goal is to fill the lumpectomy defect three dimensionally, as can be seen in his patient here:
Finally, plastic surgeon Dr. John Kim performs a latissimus procedure as a delayed revision of a lumpectomy defect for women who were treated with a lumpectomy months or years prior. Typically, these women have some scarring, dimpling or other noticeable defects that Dr. Kim is able to revise with a flap from her back, as with this particular patient:
Check out Dr. Kim’s article entitled “Latissimus Flap Breast Reconstruction” on eMedicine.com here for more on the latissimus reconstructive modality.
One disadvantage of this procedure is that it leaves patients with a scar on the back in addition to the mastectomy scar on the breast. Dr. Kim does his best to create the scar in the area covered by a bra strap. Additionally, some women report partial loss of strength or function on the side of their latissimus flap, making it hard to twist their upper bodies or lift certain things. Thus, it is generally a good idea to only have latissimus reconstruction on one side to avoid potential muscle issues on both sides. Women who are particularly active in golf, climbing, swimming, tennis or similar activities may want to consider a different reconstructive modality for their treatment.
FAQ’s Latissimus Flaps
What are the benefits of latissimus flap breast reconstruction compared to other reconstruction methods?
The latissimus flap technique uses muscle, fat, and skin from your back to reconstruct the breast. One of the key advantages is that it provides a natural tissue option without relying solely on implants. Additionally, it can be a good alternative for women who may not have enough tissue in the abdomen for other types of reconstruction, such as TRAM flaps. It’s also often preferred for patients who need additional tissue coverage or who have had prior complications with other forms of reconstruction.
How long does recovery take after latissimus flap breast reconstruction?
Recovery from latissimus flap surgery generally takes about four to six weeks, but this can vary depending on your overall health and the specifics of your surgery. In the first few weeks, you will likely experience some discomfort and limited mobility in both your chest and back. Dr. Kim will provide you with detailed post-operative care instructions to ensure a smooth recovery. You may also be referred to physical therapy to help regain strength and flexibility in your shoulder and back area.
Will the latissimus flap procedure affect my ability to lift or perform physical activities?
In most cases, patients regain full strength and mobility after recovery, but it may take time to rebuild strength in the back and shoulder area. Dr. Kim will guide you through a gradual return to physical activities, including lifting. Some patients may notice mild weakness in their back or arm on the side where the flap was taken, but this usually improves with time and proper rehabilitation.
Can the latissimus flap be combined with an implant for a larger breast size?
Yes, the latissimus flap can be combined with an implant to achieve a larger breast size or to create a more symmetrical look. The flap provides additional tissue to cover the implant, creating a more natural appearance and feel. This combined approach can be an excellent option for patients who desire larger breasts but do not have enough tissue for reconstruction with flaps alone.
What are the risks or potential complications associated with latissimus flap breast reconstruction?
As with any surgery, there are potential risks and complications, which may include infection, fluid buildup (seroma), scarring, or issues with wound healing. Specific to the latissimus flap procedure, there is a small risk of back weakness. Dr. Kim will discuss these risks in detail during your consultation and provide recommendations to minimize complications.
How does latissimus flap breast reconstruction differ from abdominal flap (TRAM) reconstruction?
The primary difference lies in the source of tissue. The latissimus flap uses muscle, skin, and fat from the upper back, while TRAM flaps use tissue from the abdomen. Abdominal flap reconstructions are often preferred for women who desire more volume, as the abdomen generally provides more fat. However, for women with insufficient abdominal tissue or those who cannot tolerate other surgeries, the latissimus flap is a reliable and shorter option.
Will I have visible scarring after the latissimus flap procedure, and how can it be minimized?
Yes, scarring is expected after surgery, with most patients having scars on their back and around the breast area. Dr. Kim takes great care to place incisions in areas that can be easily concealed by clothing or bra straps. Over time, scars typically fade, and various treatments such as silicone sheets or laser therapy can further reduce their appearance. Dr. Kim will discuss ways to minimize scarring during your post-operative care.
For more information on latissimus flap breast reconstruction, please contact board-certified reconstructive surgeon Dr. John Kim at his Chicago office today.
How does the latissimus flap procedure work?
During this procedure, a portion of your latissimus dorsi muscle, along with the skin and fat over it, is moved from your back to your chest. This tissue is shaped into a new breast mound and, if needed, combined with an implant to achieve your desired size and contour. The technique allows for reliable blood flow and optimal healing.
How should you prepare for latissimus flap breast reconstruction?

Preparing for surgery starts with a personalized consultation with Dr. Kim. During this visit, you’ll review your full medical history, discuss your goals and concerns, and undergo necessary lab work or imaging studies to assess your readiness. To prepare effectively, you should:
- Quit smoking at least several weeks prior to surgery, as smoking can significantly impair healing and increase the risk of complications Avoid blood-thinning medications and supplements like aspirin, ibuprofen, and vitamin E, as advised by Dr. Kim.
- Maintain a healthy, balanced diet to support your immune system and promote tissue recovery Arrange for assistance at home, especially for the first week post-surgery when mobility may be limited.
- Follow all detailed pre-operative instructions provided by Dr. Kim’s team, including guidelines on fasting, bathing, and medications to take or stop.
What is recovery like after latissimus flap surgery?
Recovery takes several weeks. Expect swelling, soreness, and some bruising at the donor and reconstruction sites. You’ll have surgical drains and may need a compression garment. Most patients return to light activities within two weeks and resume full activity around six weeks. Dr. Kim will guide you through each step of recovery and monitor your healing closely.
Will you need an implant with a latissimus flap?
Often, yes. The transferred back tissue alone may not be enough to achieve your desired breast volume. Adding an implant allows for better shape, projection, and balance with your natural breast or other reconstructed breast. The flap provides excellent coverage and support for the implant.
Can this type of reconstruction be done after radiation therapy?
Yes, latissimus flap reconstruction is frequently used after radiation. Radiation can damage your chest tissue, making other reconstruction methods more difficult. The latissimus flap brings healthy, non-radiated tissue into the area, improving healing and the overall outcome.
Will surgery affect your ability to lift, stretch, or exercise?
You may notice some temporary weakness or tightness in your shoulder or back. However, most people regain full mobility and strength with time and physical therapy. Long-term, this procedure typically does not limit your ability to lift or exercise.
What kind of long-term results can you expect?
Over time, your reconstructed breast will settle into a more natural look and feel. Some patients may need minor revisions, such as fat grafting or scar refinement, to fine-tune the results. Regular checkups with Dr. Kim are key to monitoring your reconstruction and maintaining your breast health.
Who is a good candidate for latissimus flap breast reconstruction?
You’re a good candidate if:
- You’ve had a mastectomy
- You need extra tissue for reconstruction
- You’ve undergone radiation
- You’re not eligible for abdominal-based flaps
- You’re in overall good health and a non-smoker
Dr. Kim will help determine if this procedure fits your individual needs and goals.