
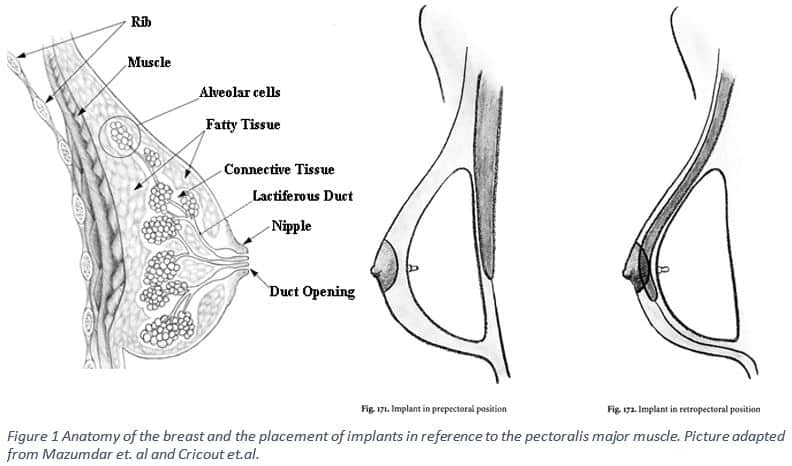
When deciding to have breast augmentation or reconstruction with Dr. John Kim at Northwestern Medical Group there are two positions where the implant can be placed that can accommodate your unique anatomy, lifestyle, cosmetic preferences, and implant type1. Implants can be placed over the pectoralis muscle (prepectoral) or beneath the muscle (subpectoral) as seen in Figure 1. Placement of the implant over the pectoralis muscle would mirror the normal anatomic position of the breast 2. In figure 1 the anatomy of the breast is represented on the left. The middle figure shows the pre pectoral arrangement, where from posterior to anterior there is the bone, pectoralis muscle, prosthetic breast tissue then skin. The picture on the right depicts the subpectoral arrangement; from posterior to anterior: bone, breast tissue, pectoralis muscle, and skin. The pectoralis muscle is a thick fan-shaped muscle, superior to the serratus anterior muscle (deep to the lower regions of breast tissue) that separates the breast from the ribs 3. Breast tissue is complex and made up of fat, connective tissue, lobes, lobules, ducts, blood vessels, nerves, and lymph nodes 3. For useful information about plastic surgery recommended by Dr. John Kim click here.
Prepectoral placement has some cosmetic issues that may require reoperation, but it avoids other undesirable outcomes. The prepectoral position of the implant can prevent issues such as breast implant animation defect, movement of the breast resulting from arm movement due to the contraction of the pectoralis muscle4. Since the implant is located over the muscle, any movement involving contraction of the pectoralis muscle will not affect the appearance of the implant. For women who are active, it is important to ask your plastic surgeon how the surgery may affect your ability to stay active. The prepectoral placement is desired when the patient would also like a breast lift with their augmentation or reconstruction 4. If the prepectoral tissues are sparse the contour of the implant can risk visibility in the upper pole of the breast and capsular contracture2,5. In a study of 200 patients who underwent subpectoral (n=100) or prepectoral (n=100) breast augmentations, the researchers found that the type of implant used would have an effect on the patients cosmetic result depending on where it was placed5. When textured saline versus silicone implants were used in the subglandular position rippling was seen5.
When the implant is placed below the pectoralis muscle there are some advantages. Deeper implant placement can help to camouflage any implant deformities as well as preventing bottoming out. Bottoming out is seen when the implant sits too low causing the nipple areola complex to tip upward and the inframammary crease to sit lower1,4. Subpectoral placement is recommended for very thin bodies, because the muscle will better conceal the edges or rippling of the implant4. The subpectoral placement may offer a better cosmetic result, although there are also some disadvantages that may require reoperation. To place the implant below the pectoralis muscle involves the partial detachment of the pectoralis muscle 1. This partial detachment can result in muscular deficit and postoperative pain1. In this placement there is also the risk of implant animation, malposition and asymmetry5.
To counteract these possible problems Reitsamer and colleagues have developed another method to overcome the issue utilizing a prepectoral placement of the implant supported with ADM. The ADM completely covers the implant including ADM coverage in the upper pole1. This allows the surgeon to overcome the possible complications associated with the subpectoral implant placement and the potential poor cosmetic result associated with prepectoral placement1. This new technique may have a permanent place in the repertoire of plastic surgeons as soon as long term testing has been completed.
The problem of implant placement is not one size fits all, and many things must be considered. When you decide to have a procedure done talk with your doctor to decide which placement will offer the best cosmetic result with the least number of complications. To see one of Dr. Kim’s publications on breast reconstruction or breast augmentation outcomes click here.
1.Reitsamer, R., & Peintinger, F. (2015). Prepectoral implant placement and complete coverage with porcine acellular dermal matrix: a new technique for direct-to-implant breast reconstruction after nipple-sparing mastectomy. Journal of Plastic, Reconstructive & Aesthetic Surgery, 68(2), 162-167.
2. Bricout, N. (1996). Pre-or retropectoral placement of the implant. In Breast surgery (pp. 205-209). Springer Paris.
3. Gray, Henry. Anatomy of the Human Body. Philadelphia: Lea & Febiger, 1918; Bartleby.com, 2000. bartleby.com/107/.
4. Madsen Jr RJ, Chim J, Ang B, Fisher O, Hansen J. Variance in the origin of the pectoralis major muscle: implications for implant-based breast reconstruction. Ann Plast Surg 2013 Sep 18.
5. Strasser, E. J. (2006). Results of subglandular versus subpectoral augmentation over time: one surgeon’s observations. Aesthetic Surgery Journal, 26(1), 45-50.
6. Mazumdar, M.D., M.D. “Breast Anatomy, Breast Cancer and Treatment.” Breast Cancer Treatment. N.p., n.d. Web. 09 Jan. 2017.