
Breast augmentation is the most frequently performed cosmetic procedure in the United States according to the American Society of Plastic Surgeons Annual Survey1. There are a number of reasons to undergo breast augmentation such as being unhappy with breast size and loss of fullness after weight loss or pregnancy to name a few. After breast augmentation, like any surgery, there is a risk of complications; to read more about complications associated with breast surgery see Dr. Kim’s CV and read one of his 172 peer reviewed publications. When the implant is placed, a capsule forms around the implant as a part of the body’s natural response to a foreign body2. This capsule is the pocket that keeps the implant in place. Although if the implants are the incorrect size or if they are placed too close to the sternum there is the possibility of displacement of the implant and capsule3.
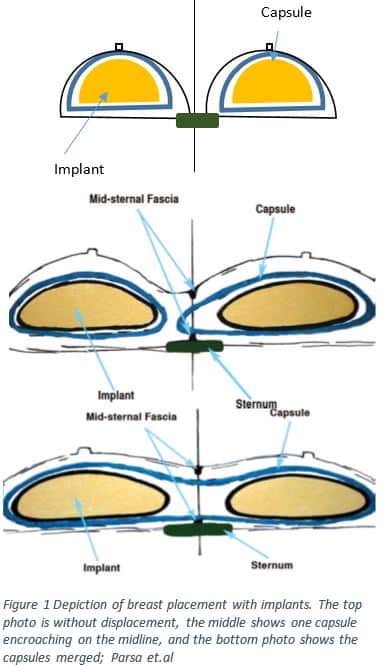
A relatively rare complication, symmastia, can occur shortly after surgery or present in a delayed fashion. Symmastia occurs when one or both the implants move toward the midline and the midsternal fascia is no longer intact, creating what looks like a “uni-boob” as seen in Figure 1. As the implant moves toward the midline the skin doesn’t adhere as tightly to the sternum4. The top image shows two implants within their respective capsules separate from the midline. In the middle image each implant is within its own capsule, some of the surrounding tissue has migrated toward the midline. In the image below both capsules have merged and created one pocket.
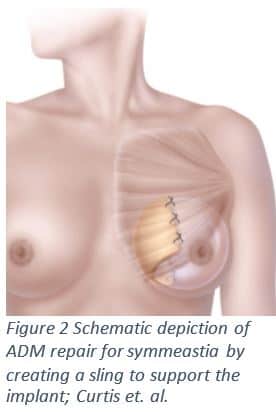
If the implant capsule does not provide enough support for the implant and symmastia results, the surgeon can perform a capsulorrhaphy to tighten and reinforce the borders of the capsule5. Symmastia may also be treated by creating a neosubpectoral pocket; a capsule that is still below the pectoralis muscle and above the old capsule6. The surgeon may also choose to reinforce the capsule using an acellular dermal matrix (ADM). The ADM is placed medially to reinforce the medial border of the capsule7,8. To see Dr. John Kim correcting symmastia with ADM click here.
In order to prevent implant displacement and symmastia it is crucial to talk to your surgeon about choosing the right size implant. Also, women with a depressed sternum are more likely to experience an implant displacement. It is important to talk to your surgeon about your goals with cosmetic enhancement. Through conversation and resources such as the 3D camera, that give the patient a virtual image of their result, the surgeon can create the new form on the patient’s individual frame.
If you are interested in undergoing a breast augmentation at Northwestern Medical Group, your surgeons will help to create the outcome you desire and manage complications that may arise. To learn more about breast augmentation click here to see an engaging 3D animation. Dr. Kim and his well-informed staff will support and guide you through the decision to have augmentation and care for any problems that may arise.
1. American Society of Plastic Surgery. (2015). 2015 Plastic Surgery Statistics Report: ASPS National Clearinghouse of Plastic Surgery Procedural Statistics. Arlington Heights, IL.
2. Rubino, C., Mazzarello, V., Farace, F., D’Andrea, F., Montella, A., Fenu, G., & Campus, G. V. (2001). Ultrastructural anatomy of contracted capsules around textured implants in augmented breasts. Annals of plastic surgery, 46(2), 95-102.
3. Chang, S., Gowda, A., Mavrophilipos, V., Semsarzadeh, N., & Singh, D. P. (2014). Common Complications in Aesthetic Breast Augmentation. Eplasty, 15, ic49-ic49.
4. Parsa, F. D., Koehler, S. D., Parsa, A. A., Murariu, D., & Daher, P. (2011). Symmastia after breast augmentation. Plastic and reconstructive surgery, 127(3), 63e-65e.
5. Harris, R., Raphael, P., & Harris, S. W. (2014). Thermal capsulorrhaphy: a modified technique for breast pocket revision. Aesthetic Surgery Journal, 34(7), 1041-1049.
6. Spear, S. L., Dayan, J. H., Bogue, D., Clemens, M. W., Newman, M., Teitelbaum, S., & Maxwell, G. P. (2009). The “neosubpectoral” pocket for the correction of symmastia. Plastic and reconstructive surgery, 124(3), 695-703.
7. Slavin, S. A., & Lin, S. J. (2012). The use of acellular dermal matrices in revisional breast reconstruction. Plastic and reconstructive surgery, 130(5S-2), 70S-85S.
8. Curtis, M. S., Mahmood, F., Nguyen, M. D., & Lee, B. T. (2010). Use of AlloDerm for correction of symmastia. Plastic and reconstructive surgery, 126(4), 192e-193e.